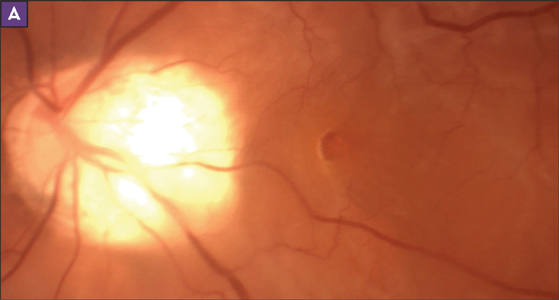
MHRD - Macular Hole Retinal Detachment
- Asymptomatic Macular holes in myopes – 6.28%
- Asymptomatic nature – Juxtafoveal location
- Risk Factors for evolution to Symptomatic MH ± RD – younger age, higher degree of myopia, presence of epiretinal tissue
- MH ± RD – not uncommon in high myopes; especially associated with posterior staphyloma
- Incidence of RD in MH increases from 0.6% overall to 10% in high myopes.
Epidemiology
- Age – 52 yrs
- Sex – 66% females
- Axial Length – 28.1mm
- Refractive Error - -12D.
- Configuration of RD – Inferiorly Bullous
- Pre-op inability to identify MH on biomicroscopy – 33% (lack of contrast, posterior staphyloma, severe CR atrophy)
Etiopathogenesis
- Abnormal vitreous and vitreo-retinal interface in myopes
- Role of Antero-posterior and tangential traction – causation of myopic MH
- Role of inverse retinal traction – causation of myopic MHRD
Treatment
- Episcleral macular buckling
- Pneumatic Retinopexy
- PPV with partial fluid-air exchange
- PPV with long acting intraocular gas tamponade
- PPV + ERT/residual cortical vitreous/ILM peeling + gas tamponade
- PPV + ERT/ILM peel + silicone oil tamponade ± laser photocoagulation
- compiled & published by Dr Dhaval Patel MD AIIMS
